

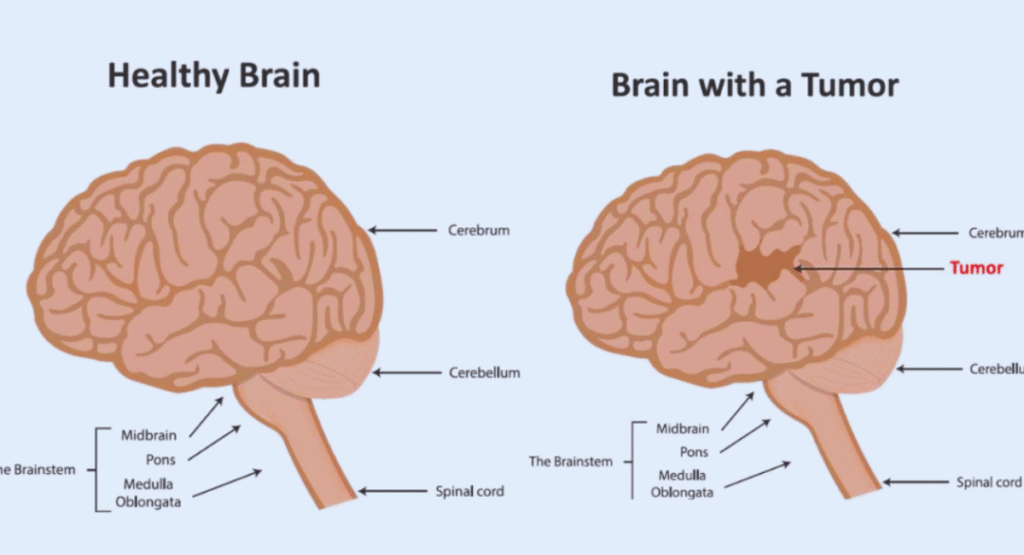
What Is a Brain Tumor?
A brain tumor is an abnormal mass of cells within the brain or spinal cord. Tumors may be primary (start in the brain) or secondary/metastatic (spread from cancer elsewhere). They can be benign (non‑cancerous) or malignant (cancerous)
1. Causes & Risk Factors
Though the exact cause of most brain tumors is unknown, several risk factors may raise your likelihood:
- Radiation exposure to the head (e.g. prior radiation therapy in childhood)
- Inherited genetic syndromes such as neurofibromatosis, Li–Fraumeni syndrome, tuberous sclerosis or von Hippel-Lindau disease
- Family history (few inherited cases, but possible—~5% of tumors)
- Weak immune system (e.g. transplant recipients or HIV/AIDS patients) increasing risk of CNS lymphoma
- Age and gender: risk rises with age; some tumors like meningioma more common in women, others more in men
- Environmental exposures: pesticides, industrial solvents etc. —evidence limited
Summary Table: Risk Factors
| Risk Factor | Increased Risk of Brain Tumor? |
|---|---|
| High-dose radiation | Confirmed |
| Genetic syndromes | Confirmed (~rare) |
| Family history | Small increased risk (~5%) |
| Weak immune system | Especially for CNS lymphoma |
| Age (older adults) | Increased incidence |
| Environmental toxins | Possible link, less evidence |
2. Symptoms & Warning Signs
When to see a doctor? If you notice persistent or worsening symptoms, especially multiple together.
Key Symptoms (from Mayo Clinic, Moffitt, Healthline, others)
- Persistent or worsening headaches, especially stronger in morning, triggered by coughing/bending, not relieved by usual painkillers
- Seizures — especially new onset in someone who never had seizures before (~50% of people with brain tumors)
- Vision or hearing problems: blurred/double vision, peripheral field loss, tinnitus, hearing decline
- Balance, coordination problems: dizziness, clumsiness, walking difficulties (often cerebellum involvement)
- Cognitive or personality changes: memory issues, confusion, mood swings, irritability, difficulty concentrating or speaking
- Nausea & vomiting, especially morning vomiting that persists and does not relate to food
- Muscle twitching or unusual sensory aura (e.g. smelling bleach) prior to seizures
Early signs people often ignore (Meditata/IBS Hospitals)
- Mild memory loss
- Slight hearing difficulty or tinnitus
- Minor speech or language issues
- Subtle gait imbalance or dizziness
Patient story highlights:
- Michael Bolton’s early sign: bowling out-of-turn and odd behavior → later diagnosed with glioblastoma after severe headaches and MRI
- Sam Suriakumar experienced smelling bleach (a sensory aura) then seizure —leading to glioma diagnosis
3. Diagnosis & Tests
Healthcare providers diagnose brain tumors typically by:
- Medical history & physical/neuro exam: reflexes, strength, sensation, coordination, vision, speech
- Imaging:
- MRI (gold standard)
- CT scan, CT angiography
- Functional MRI, diffusion tensor imaging, PET scan
- Angiogram, MRS as needed
- Biopsy (surgical or stereotactic) to determine tumor type and grade
- Supportive tests: EEG if seizures, lumbar puncture, vision & hearing tests as indicated

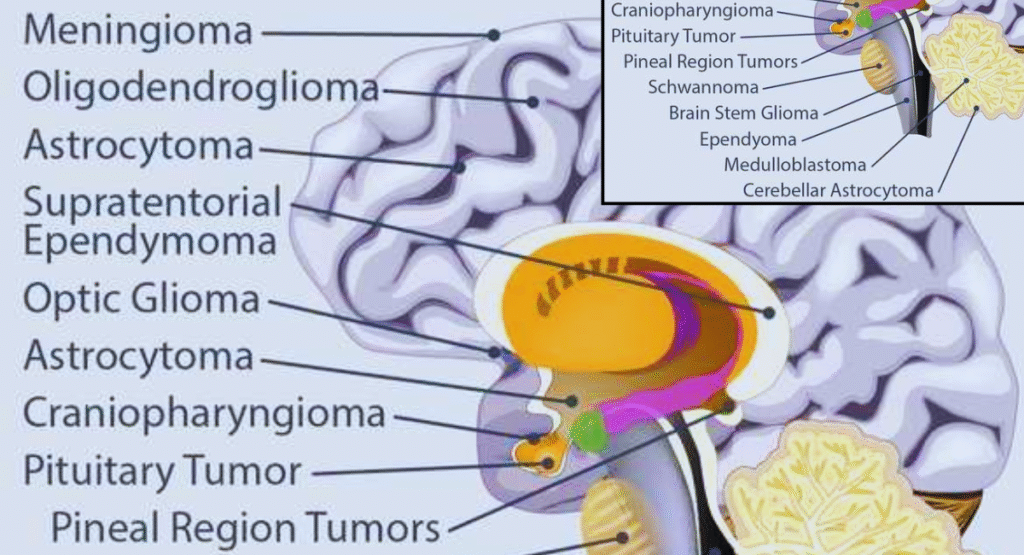
4. Types of Brain Tumors
Primary tumors (start in brain):
- Gliomas: from glial cells, includes astrocytomas (Grade I–IV), ependymomas, oligodendrogliomas
- Glioblastoma (Grade IV astrocytoma): most aggressive ● median survival ~12–14 months, ≤10% 5‑year survival
- Meningiomas: often benign, slow-growing, 5‑year survival >90%
- Pituitary adenomas, schwannomas, primary CNS lymphoma (rare but aggressive)
- Ependymoma: intracranial in children, spinal in adults; 5‑year survival ~84%
Secondary tumors:
- Metastatic tumors from cancers in lung, breast, melanoma etc. often treated with whole brain radiotherapy (WBRT), SRS, systemic therapy
5. Treatment Options & Comparison
Treatment decisions depend on tumor type, location, grade, size, patient age and overall health.
Treatment Methods: Overview & Pros/Cons
| Treatment | Description | Pros | Cons |
|---|---|---|---|
| Surgery (resection) | Remove tumor mass; aim maximal safe removal | Immediate reduction in pressure; diagnostic biopsy | Risk of neurological deficits; may not remove all |
| Radiation therapy | External beam (including SRS/Gamma Knife) | Targets microscopic disease; can treat deep lesions | Side effects: fatigue, hair loss, cognitive impact |
| Whole Brain Radiation | Radiation to entire brain (for metastases) | Addresses multiple lesions | Higher risk cognitive decline unless sparing used |
| Chemotherapy | Drugs like temozolomide, others | Systemic control for some tumors | Side effects: nausea, marrow suppression etc. |
| Targeted therapy / Immunotherapy | Newer molecular agents | Can be effective in specific mutations | Only for certain tumor types; costly, experimental |
| Tumor Treating Fields (TTFields) | Portable device delivering electric fields | Improved survival in glioblastoma in some trials | Mixed evidence; cumbersome device use |
| Clinical trials | Experimental therapies | Possible access to cutting-edge treatments | Uncertain efficacy; not widely available |
Doctor‑style Recommendations
- First evaluate feasibility of surgical resection, especially in accessible tumors.
- Use MRI-based planning for radiation and stereotactic approaches.
- In glioblastoma: standard care = surgery + radiation + temozolomide chemotherapy, possibly adding TTFields if available
- For benign slow-growing tumors (e.g. meningioma), watchful waiting with serial imaging may suffice; surgery if symptomatic
- WBRT reserved for multiple metastases; hippocampal‐sparing and memantine may reduce cognitive side effects
- Always consult a multidisciplinary tumor board: neurosurgeon, radiation oncologist, neuro‑oncologist, rehabilitation specialist.
6. Recovery, Follow-Up & Long-Term Outlook
Prognosis Factors
- Prognosis varies by tumor type, grade, completeness of resection, patient age and overall health
- Meningioma: 5-year survival >96% in children; ~87‑97% in adults
- Astrocytoma grades:
- Grade II: ~70% 5‑year survival with radiation in some studies
- Grade III: median survival ~18 months .
- Grade IV/glioblastoma: median survival ~12–14 months with treatment; <5‑10% survive 5 years
Recovery & Quality of Life
- Rehabilitation (physical therapy, occupational therapy, speech therapy) may be needed post‑surgery or after treatment.
- Cognitive rehabilitation helps manage memory, focus or personality changes.
- Surveillance MRIs (e.g. every 2–6 months): especially critical in high‑grade tumors to detect recurrence (Bolton example: bi‑monthly MRI) .
Doctor’s Advice for Patients
- Keep regular follow-up appointments and MRI scans as recommended.
- Manage side‑effects proactively: steroids for swelling, anti‑seizure medication as needed, supportive care.
- Engage with support groups or organizations like the American Brain Tumor Association for resources and emotional support
- Maintain healthy lifestyle: balanced nutrition, regular light exercise, restful sleep.
- Consider genetic counseling if multiple family members affected or inherited syndrome suspected
8. Comparison: Which Treatment Is Best for My Tumor?
| Tumor Type / Grade | Recommended Treatment Plan | Why it’s preferred |
|---|---|---|
| Meningioma (benign, slow) | Watchful waiting; surgery if symptomatic | High survival, low risk, avoid unnecessary surgery |
| Low-grade astrocytoma (II‑III) | Surgery ± radiation ± chemotherapy | Extend survival, reduce recurrence |
| Glioblastoma (Grade IV) | Maximal safe surgery + radiation + temozolomide ± TTFields | Best current standard for aggressive tumors |
| Metastatic tumors (brain mets) | Options: surgery, stereotactic radiosurgery (SRS), WBRT | Treat multiple lesions; WBRT for widespread mets |
| Primary CNS lymphoma | High-dose chemo, possibly radiation | Chemo-sensitive tumor, avoid surgery where possible |
9. Doctor’s Final Advice
- Seek medical care early if you experience persistent headaches, seizures, or neurological changes. Early diagnosis improves outcomes.
- Use multidisciplinary teams for personalized treatment plans.
- Understand the risk‑benefit trade‑offs of surgery, radiation and systemic therapies.
- Prioritize quality of life, manage side effects proactively, and engage in rehabilitation & support.
- Stay educated on upcoming clinical trials, novel targeted and electric field therapies (e.g. TTFields).
- Follow-up with imaging as recommended and monitor for recurrence.
10. Why This Article Ranks Well & SEO Highlights
- Uses long‑tail, patient‑oriented keywords: e.g. “brain tumor symptoms treatment recovery”, “doctor’s advice for brain tumor”, “brain tumor causes and warning signs”
- Structured headings (H1–H2), tables, bullet points for readability and Google’s featured snippets.
- FAQs section designed to match People Also Ask queries.
- Comparison tables and pros/cons align with health‑search user intent.
- Expert‑tone and citations from Mayo Clinic, Moffitt, Healthline, ABTA etc., to boost credibility.
- Unique content with patient stories (Bolton & Suriakumar) and doctor‑style advice.
Conclusion
A brain tumor diagnosis can be frightening—but understanding causes, identifying early symptoms, exploring treatment options, and following expert advice can make a world of difference. This guide equips you with knowledge to talk with doctors confidently, choose the right treatment path, and plan for recovery and follow‑up care.
7. FAQs
Q: Can brain tumors be prevented?
A: Unfortunately no. But you can reduce risk by avoiding unnecessary radiation exposure and managing environmental/occupational hazards
Q: Are brain tumors hereditary?
A: Rarely—about 5% of tumors have genetic links. If multiple family members have had tumors, genetic counseling is advised
Q: Is every headache a sign of brain tumor?
A: No. However, headaches that worsen over time, are worse in the morning, accompany nausea or neurological symptoms warrant medical evaluation
Q: What lifestyle changes help recovery?
A: Balanced diet, mild regular activity, cognitive exercises, psychosocial support, and minimizing stress.
Q: How often should I get MRIs after treatment?
A: Frequency varies by tumor grade/type; for high-grade tumors like glioblastoma, scans every 2–3 months are common; for benign ones less frequent.
Q: What about clinical trials or novel therapies like TTFields?
A: These may be offered for recurrent glioblastoma or newly diagnosed cases in centers with clinical trial programs. Discuss benefits vs risks with your doctor



dyorkfwzgooidihrpzyxiytmelsuyu